AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2578-8949/039
*Corresponding Author: Hilde H. Buzzá, São Carlos Institute of Physics, University of São Paulo (USP),Brazil
Citation: Hilde H. Buzzá, Mirian D. Stringasci1, Cintia T. Andrade2, Ana G. Salvio3, Expanding dermatologists view with fluorescence and thermograph J.Dermatology and Dermatitis, DOI : 10.31579/2578-8949/039
Copyright: © 2018 Hilde H. Buzzá et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 May 2018 | Accepted: 30 June 2018 | Published: 09 July 2018
Keywords: Fluorescence; Thermograph; Endogenous Fluorescence; Marked fluorescence; skin lesions.
Several skin lesions are characterized as public health problem due their high incidence. Some lesions denominated premalignant have the potential to progress to malignant lesions and the treatments can have great successful rates if it has a right and precise indication. Diagnosis depends on the experience of the physician to identify tissue changes, mainly in the early stages due to the similar clinical characteristics among different types of lesions. Therefore, the interest in noninvasive diagnosis techniques and not harmful to health is increasing. This study shows tools for skin lesions application complementing the initial clinical examination with fluorescence and thermograph methods. The fluorescence evaluation was performed using a device for the wide field image for the evidentiation of endogenous fluorescence and following Photodynamic Therapy with marked fluorescence. Infrared images were obtained using a thermal camera. Endogenous fluorescence diagnosis can improve the visual contrast between normal and abnormal tissue, contributing to biopsy site determination, lesion border delimitation and lesion identification, such as melanoma and pigmented seborrheic keratosis. Marked fluorescence with Protoporphyrin IX was used to check whether the treatment was as expected and can be used to increase the successful of results. Thermograph was used to discriminate lesions clinically similar, such as actinic keratoses and squamous cell carcinoma that can be simultaneously present, because AK is transformed in SCC in a continuous and progressive process. Fluorescence and thermograph were used to lesion discrimination, border identification and monitoring treatments enabling the physician to indicate the procedure with more confidence.
Among all types of cancer, the highest incidence in the world is the skin cancer, which 95% are non-melanoma lesions and its more common forms are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). The exposure to ultraviolet (UV) radiation from sunlight is a major known risk factor for the non-melanoma skin cancer development. (1) Melanoma is the most invasive and aggressive type of skin cancer and, despite representing only 3% of incidence, it is responsible for about 65% of deaths. It can be clinically similar to pigmented seborrheic keratosis (PSK), which is a benign lesion (2,3).
Some lesions denominated premalignant have the potential to progress to malignant lesions. Actinic keratoses (AK) are one of the most incident ones and they are frequent in 60% of patients aged over 40 years, affecting, usually, the body areas most exposed to solar radiation. (4) Nearly 60% of SCCs is originated by AKs and the progression rate from AKs to SCCs varies from 4 to 16% a year (5). Early stages diagnosis of SCCs is important because it is responsible for 34% of deaths caused by skin cancer around the world (6).
The treatment will have great successful rates if it has a right and precise indication and, for this, it is necessary to determine clinical and histopathological characteristics of the lesion. That information ensures the therapeutic adequacy and individualization for each patient and it is resulting from several procedures, such as the search of patient record or clinic examination with visual analysis and palpation. Also, there are laboratory tests as cytology, biopsy and biochemical tests or imaging tests as X-ray or Magnetic Resonance Image (7). The following of treatments and the guarantee of the procedure were as expected with the exact diagnosis of disease are two of main requirements for a good clinical conduct. Photodynamic Therapy (PDT) is an alternative treatment with light that has been largely used in skin disorders(8).
Laser and optical fibers made possible the disease diagnosis with light, replacing highly invasive and mutilating procedures. Techniques with the wide-field image, optical coherence tomography, confocal microscopy and diagnostic by fluorescence are some examples of techniques with light to identify several diseases.
Fluorescence occurs when an atom absorbs an incident light of a certain wavelength and goes from the ground state (lowest energy) to an excited state (higher energy), which is unstable, thus the atom tries to return to the ground state. For this, the atom has to re-emit the absorbed energy, which decreased in the amount due to energy losses that occur inside the molecule. The emitted light (fluorescence) has, then, a longer wavelength that means a different color of absorbed light. Fluorescence characterizes the chemical and physical changes occurring in tissue since each difference will mean different energy losses and wavelength re-emitted. Thus, different tissues or different conditions of the same tissue have distinct endogenous fluorescence (9) and can be used as a detection method to improve the accuracy in diagnosis. The improvement can be by both helping the physician to differentiate types of lesions and allowing lesion borders delimitation, which could provide a most specific treatment, avoiding big surgery or remaining abnormal cells.
Another parameter that can be evaluated is the tissue temperature, which is influenced by blood perfusion and metabolic rate. A tissue with lesion has those characteristics different from a normal one, because its growth and consequent need for nutrient are higher, stimulating angiogenesis (10–12).The thermograph records a body temperature distribution using the infrared radiation emitted by the surface of this body, with a wavelength between 7 and 14 µm(13).
From several studies that have been conducted at the Skin Department of Amaral Carvalho Hospital Foundation in Jahu – SP, Brazil and Brazilian Program of Photodynamic Therapy, images of skin lesions were recorded, analyzed and compared with the diagnosis set by the physician and by histopathology. Eligible patients were subjects of both genders, over 18 years old with different lesions, such as primary superficial (sBCC), nodular (nBCC), or pigmented (pBCC) with a diameter less than of 20 mm, estimated clinically immediately prior to treatment, or AK, PSK, and melanoma. Pregnant always were excluded and all patients signed a written informed consent form.
The interest in these diagnosis ways is increasing, because they are noninvasive techniques and are completely not harmful to health. This report aimed to show tools for skin lesions application complementing the initial clinical examination with fluorescence and thermograph methods, gathering techniques already used with some applications little explored in the clinic. Despite many techniques available to use in dermatology, some techniques are easy to apply, non-invasive and multi-functions and are not frequently used by health professionals.
We are exploring especially fluorescence and thermography and the devices used by our group at São Carlos Institute of Physics and Skin Department of Amaral Carvalho Hospital Foundation in Jahu – SP.
The endogenous fluorescence evaluation could be performed using a device for wide-field fluorescence, LINCE® (MMOptics, São Carlos, Brazil). This equipment is composed of a set of LED arrays with emission in the UV-blue range of light (400 ± 10 nm) and irradiance around 50 mW/cm2. The optical arrangement allows the fluorescence viewing in a contrast visualization between colors and intensities of light in green and red. Health tissue emits fluorescence in the green region of the electromagnetic spectrum with excitation at 400 nm, due to the collagen fibers highly organized and the emission of some molecules such as NAD(H) and FAD(H) (12) while the characteristic protoporphyrin IX (PpIX) fluorescence is red. A digital color camera was coupled at the device with an adapter for image acquisition (14,15).
Figure 1 shows wide-field images from an AK in the left forearm. Figure 1-A is the white light picture where the determination of the lesion borders is difficult to establish by a non-specialist. However, the fluorescence image (Figure 1-B) allows the delimitation of the lesion borders due to the difference in fluorescence between the lesion and normal tissue, since the AK region is lighter than surroundings.

Another possibility is the use of fluorescence in discrimination of clinically similar lesions. PSK is a benign lesion that sometimes, even for the expert dermatologist, is very similar to melanoma, which is the most dangerous skin cancer (3). PSK has some tissue structures, as the corneal pseudocysts, that present different
fluorescence compared to the abnormal tissue and some light spots become evident in the fluorescence image inside of a dark area that is the lesion (Figure 2-A). Thus, this technique helps to differentiate between these two types of lesion, since the fluorescence image of melanoma is a dark area without any fluorescent spots (Figure 2-B) (15,16).

The interaction among light in a specific wavelength, a photosensitive compound (PS) and oxygen results in the cell death and characterize the principle of PDT. The main PS currently used in clinical application is the porphyrin, which accumulates mainly in modified cells and emits in the red region contrasting with the green of the health tissue.
In the Project “Photodynamic Therapy Brazil”, with national coverage, a protocol of non-melanoma skin cancer treatment was established to superficial basal cell carcinoma (sBCC) up to 2 cm in length and nodular basal cell carcinoma (nBCC) less than 2 mm in infiltration. For the treatment, the topic application was used with a cream containing the prodrug methyl aminolevulinate (MAL), the precursor of PpIX, which is an endogenous PS produced by the cells and has the fluorescence emitting in red when excited with blue light (17,18).
Therefore, the evidentiation was performed before the cream application, before the illumination to verify the production and accumulation of PS, and immediately after PDT to confirm the bleaching of PpIX showing to the health professional that the illumination occurred in the right place and with the expected dose (4).
The following of PDT over time in a sBCC is showed in Figure 3, after the incubation time (Figure 3-A) and after the illumination (Figure 3-B), showing almost all PpIX consumed.

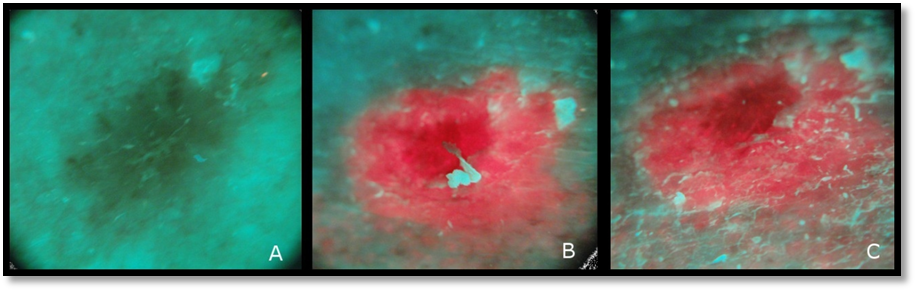
However, there are some cases where the illumination happened in a non-efficient way and the PpIX is not consumed. Figure 4 shows the endogenous fluorescence before the cream application (Figure 4-A), after incubation (Figure 4-B) presenting a high red fluorescence indicating a PpIX production and after PDT (Figure 4-C), showing there is still a lot of this red fluorescence.
Infrared images can be obtained using the thermal imager (Fluke® FLK-Ti400 model), with thermal sensitivity ≤ 0.05 ° C and 320 x 240 pixels resolution. The imager has the advantage that shows the thermal image on its display without the need for coupling to a computer and has also auto focus adjustment. The visible light and thermal image are registered simultaneously and can be downloaded on the computer through its software Fluke SmartView 3.5 with color legend corresponding to temperatures.
The AK and SCC lesions can be clinically similar and are showed in the white light images, Figures 5-B and 5-D, respectively. The SCC region usually shows a significant increase of the temperature relative to healthy tissue in the thermal image (Figure 5-A) while in AK the temperature difference in relation to the surround region is less evident (Figure 5-C). This difference could be used to distinguish the type of lesions.

Diagnosis depends on the experience of the physician to identify tissue changes, mainly in the early stages of the lesion due to the similar clinical characteristics among different types of lesions. Although the clinical diagnosis of a PSK presents no difficulty, there are still some lesions that may be clinically similar to melanoma. For dermatologists, the differentiation of suspicious lesions is most of the time easily performed due to their specific training. On the other hand, for the general clinician or less experienced practitioner, this task could be more difficult.
PSK has structures correspondent to corneal pseudo cysts which, when viewed in dermoscopy are considered pathognomonic of this disease and, histologically, it is known that pseudocysts are filled with horny keratin, a highly fluorescent biomolecule when excited by 408 nm. (19–21) The fluorescence visualization provides a higher contrast to identify these structures showing some light spots in the fluorescence image. Therefore, the keratin fluorescence contrasts with the lack of fluorescence in the melanoma, visualized as a black area, due to the high melanin content that absorbs the most part of the light. Differentiating melanoma from PSK helps speed up the treatment of the higher risk lesion to the patient since corneal pseudocysts are not observed in the endogenous fluorescence of pigmented skin lesions, it may be considered of risk and be a priority for treatment.
Fluorescence also could be used to determine border of different types of lesions. Nowadays, the gold standard for diagnosis is biopsy, which is invasive and usually needs time for the result; however, if the procedure is performed on the right site, the result has accuracy (22).Endogenous fluorescence diagnosis can improve the visual contrast between normal and abnormal tissue, contributing to biopsy site determination, lesion border delimitation before treatment and lesion identification. (15,16) .The choice of the skin region that will be taken biopsy has fundamental importance, once the wrong place is chosen, the result may be a false negative, preventing the treatment of lesions in early stages.
The delimitation of the lesion border, on the other hand, contributes to choosing the safety margin, avoiding mutilating surgeries and compromised margins, which leads to the second round of treatment. This type of diagnosis helps the physician to guarantee more efficiency in the surgery.
In addition to the lesion identification, check whether the treatment was as expected is an alternative to increase the successful of results. Figures 3 and 4 showed different lesions treated with PDT and the difference between both procedures is clear. The first one is an example of efficient illumination and the last one shows a possibility of a problem during the treatment. It is clear that PpIX was not degraded for some reason during the illumination process.
This can happen, for example, when the illumination tip slid because the patient moved for some discomfort or the lesion site allowed a not good accommodation. If there is no full-time conference that the illumination is performing in the exact site, the red fluorescence will become clear in the end of PDT, which can indicate the physicist needs to repeat or change the procedure.
Monitoring PDT by fluorescence image, therefore, means an extension of the dermatologist view in a technique increasingly used in skin diseases, such as non-melanoma skin cancer or precancerous lesions.
Besides optical images, thermal images can also be used to extend the physician view. There is a difficulty in discriminating lesions clinically similar, such as AK and SCC that can be simultaneously present, because AK is transformed in SCC in a continuous and progressive process. (23–25)
In the thermal images, SCC usually presents a higher temperature compared to normal tissue, probably due to its more invasive characteristics as fast growth and high aggressively that increase its vascularization. (23) AK presented the temperature map similar to the size of the lesion and they showed no great difference of temperature in comparison with healthy tissue.
Summarizing different techniques and their application, Table 1 was done.

Lesion discrimination, border identification, and monitoring treatments may enable the physician to indicate the procedure with more confidence. Therefore, it is possible to ensure the treatment efficiency applied in any disease. About dermatology, the skin is the site of easier access to photonic and thermal techniques, opening several possibilities for both therapies and diagnosis presented in this study.
The authors acknowledge Professors Vanderlei Bagnato and Cristina Kurachi and financial support by BNDES (09.2.1458.1) and MMOptics. We appreciate the support from FAPESP (Program CEPID-INCT), CNPq, CAPES, and FINEP.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.





























































